

A FEW WORDS... Ultrasounding the chest in dyspnoea (from Ep 6)
- Feb 20
- 5 min read
Updated: Mar 28

Ultrasound—whether you’re scanning the thorax or the abdomen—is really about answering a series of simple, clinically useful yes/no questions.
As your skills improve, the number of questions you can confidently answer grows.
We’ll cover abdominal ultrasound in more detail in future guidelines. But for now… let’s focus on thoracic ultrasound.
Is this dyspnoea primarily a respiratory problem or primarily a heart problem?
Is there fluid?
Do I need to tap something?
Do I need diuretics?
This is where T-POCUS (Thoracic Point-of-Care Ultrasound) will be your saviour.
Not fancy.
Not specialist-level.
Just useful information, fast, that actually changes what you do next.
---
What is T-POCUS?
T-POCUS is a quick, targeted thoracic ultrasound that's not meant to be too technical:
Patient standing or sternal
It will go better and be less stressful with butorphanol (or stronger opioid if pain is present) upto 0.3-0.4mg/kg IV or IM.
Minimal clipping, a lot can be achieved by parting the fur
Provide oxygen by mask or flow-by if tolerated.
Apply spirit, then gel generously
Pop a lubricated ultrasound cover, or even a condom, or the finger of a disposable glove over the probe
Use your abdominal probe if you are more familiar with that.
It’s not about perfect images.
That’s it. No dissertations required.
---
What T-POCUS is not
Let’s clear this up early, because this is where people get stuck.
T-POCUS is not:
A full echocardiogram
A replacement for a cardiologist
Something you need a £70k machine for
Something you must be “certified” to attempt
You are not diagnosing mitral valve disease, or evidencing regurgitation at the mitral valve. You are not measuring fractional shortening.
Essentially, you are deciding:
Is there fluid:
in the lungs (pulmonary edema)? Diuretics needed.
floating around the lungs (pleural effusion)? Thoracocentesis needed.
around the heart within the pericardial sac (pericardial effusion)? Pericardiocentesis needed.
Is the left atrium very big? Dyspnoea is likely cardiac in origin
How well is the heart beating? Pimobendan may benefit the patient if the heart contractions are very weak.
---
The Big 3 Things T-POCUS Tells You (Very Quickly)
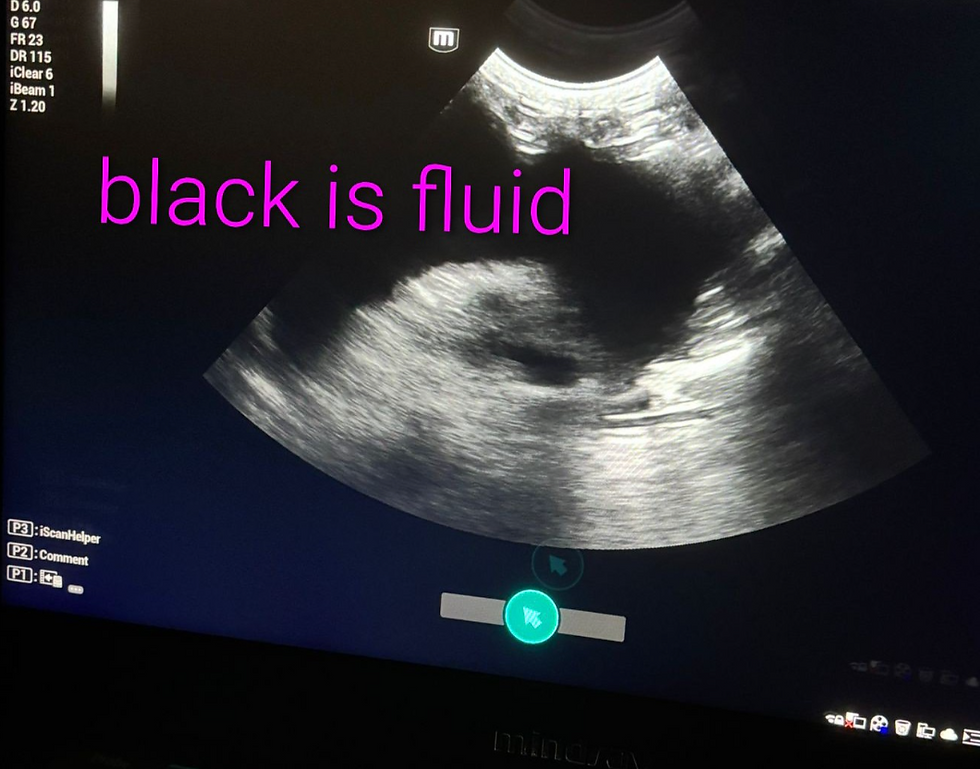
1️⃣ Pleural space: lots of fluid?
If you see:
Black fluid below the ribs with things floating around, such as a floaty white membrane.
And suddenly thoracocentesis becomes an obvious next step rather than a scary one.
---
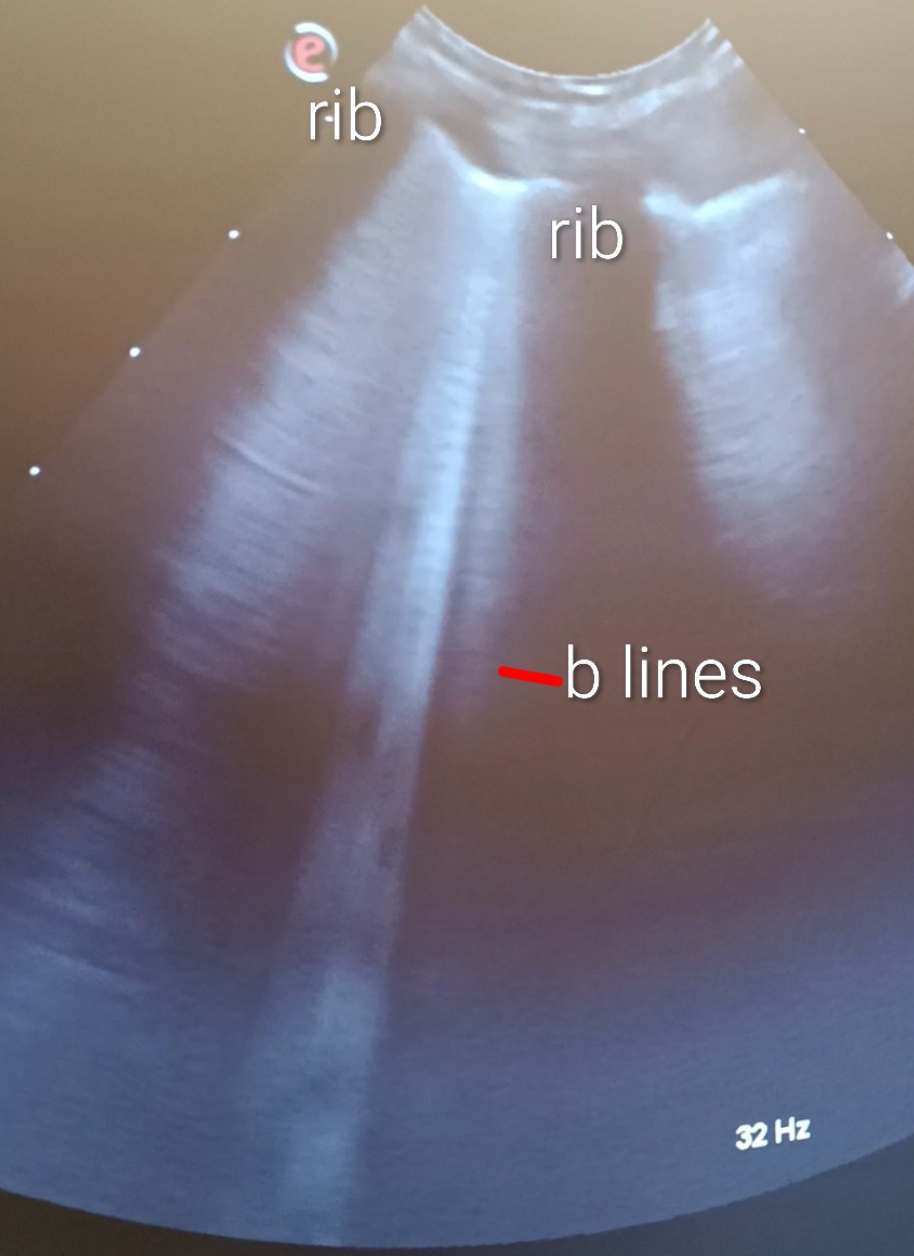
2️⃣ What are B-lines?
This is the bit that sounds scary but really isn’t. Let's start with A lines.
A-lines = air, normal lung surface.
There is a strong white line just deep to the ribs, which look like black circles, or alligator's eyes.
Horizontal reverberation lines (like an echo) due to the initial strong reflection of the beam as it hits the interface or junction between lovely air-filled normal lungs and chest wall.
Remember, the beam gets reflected by changes in density. A big density change such as soft tissue to air or soft tissue to bladder stones gets a BIG reflection.
The horizontal lines appear at intervals further down the screen as a reverberation artifact.
These lines are normal. It means we have nice, air-filled, happy lungs.
B-lines = wet lung (alveolar fluid)
These are torch lights through fog running vertically down the screen. Sometimes they seem like lasers that shoot down the screen.
They also move to and fro (side to side) with the same rhythm as the breathing.
They can be very variable in width but are usually at least several mm’s, and a grey-white colour.
More than three in a field of view is significant.
What do wet lungs mean?
Well, in a cat, this is likely cardiogenic pulmonary oedema, and we are normally checking for a big left atrium to substantiate this.
We didn’t touch on non-cardiogenic pulmonary oedema (NCPE/NCPO) in the podcast, which is worth mentioning now.
In cats especially, we often see an acute, dramatic and typically short-lived presentation of pulmonary oedema without evidence of underlying cardiac disease or other issues. These cases can look almost allergic in onset, but are more likely related to neurogenic or inflammatory increases in pulmonary capillary permeability.
The reassuring part is that many of these cases respond well to supportive care (oxygen and furosemide) and can be surprisingly transient.
Other recognised NCPE causes include pancreatitis, electrocution and seizures, which are well described but thankfully uncommon.
Pneumonia is possible, though more common in young brachy dogs than cats, or if oesophageal disease is present (megaesophagus) due to regurgitation.
---
3️⃣ Heart: big problem or small player?
A useful trick if scanning the heart in sternal:
Cup the sternum with your free hand and pull it to the left, such that you tilt the cat 10–20° so the heart falls toward the right chest wall
You’re looking for:
Put the probe against the right chest wall, about where the right elbow would be, or where you can feel the heart beating with your finger. You may need somebody very gently pulling the right foreleg forwards.
Firstly, try to find the left atrium. It's usually about one rib space cranial to the ventricles.
You are trying to see the black thin-walled atria at the top of the thicker-walled beating ventricles. I think the left atrium has a whale shape, a black ball with a tail, and adjacent, you will often clearly see a black circle about 1cm diameter in cats, which is the aorta. Closer to the top of the screen, above and wrapping around the aorta is the right ventricular outflow tract. Don't worry about this too much for now.
Just remember, you ideally take measurements when the aortic valve is closed, so you can see the Mercedes Benz sign with the valve leaflets meeting in the middle. And in a straight line avoiding measuring the appendage (tail) of the left atrium.
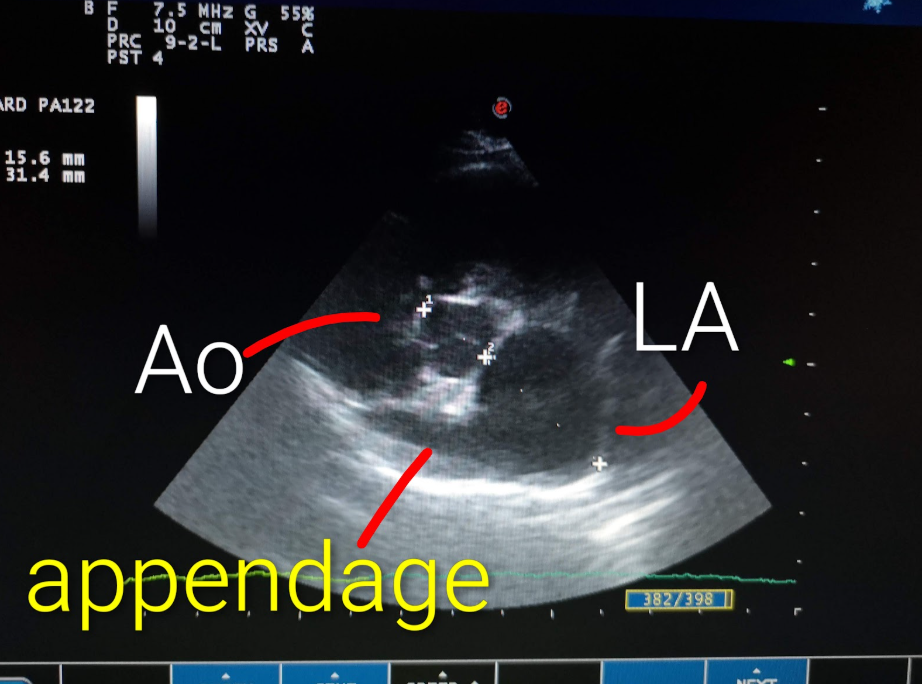
If the left atrium in a cat is moderately enlarged, about twice the diameter of the aorta or more, then CHF is the likely cause of wet lungs or pleural effusion. Just remember, dogs can be more subtle and mild left atrial enlargement can cause CHF in dogs.
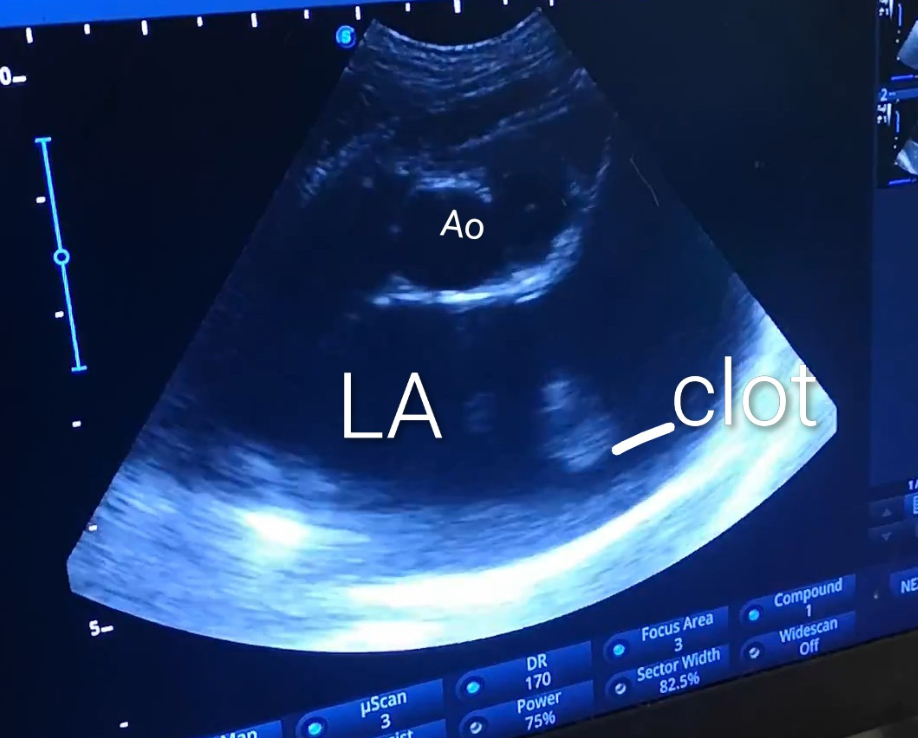
On rare occasions, blood clots can be seen swirling within a markedly enlarged left atrium. Sometimes this looks like smoke too.
---
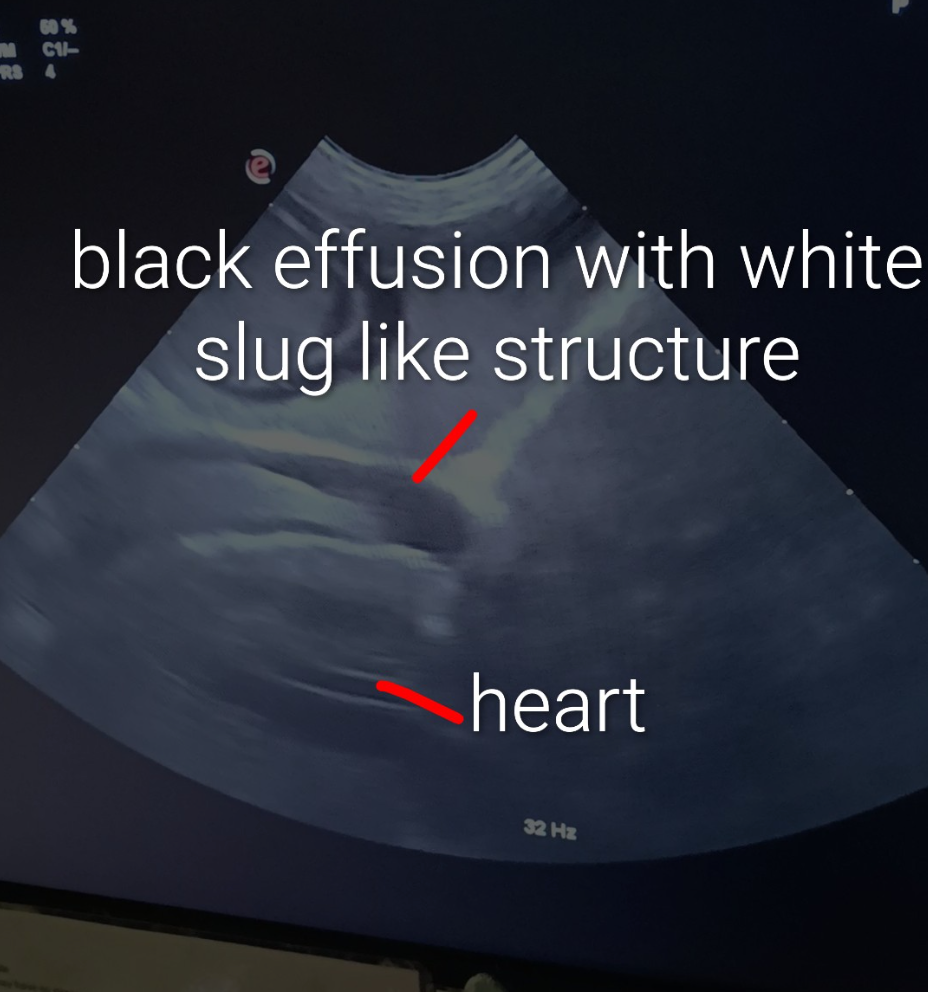
A word about pericardial effusion
It can occur in dogs and cats. In cats, they are usually milder and, in my caseload, almost incidental to finding CHF. Treatment has been with diuretics. In dogs, they are more likely to be causing a life-threatening tamponade, severely compromising cardiac function and usually need urgent drainage.
Here's an example of pericardial effusion below. In real life, it's even easier to identify as the heart is pumping away too. This particular effusion was highly unusual, because a big white slug was present within the pericardial fluid. If anyone can tell me what this was, I'll be delighted to know! Email me at hello@chattyvets.com.
Why GP vets should care (even if ultrasound scares you)
Because T-POCUS:
Takes 2–5 minutes
Works with basic machines
Reduces guesswork
---
Real talk: common worries we hear
> “I’m scared I’ll miss something.”
You already miss things without ultrasound.
T-POCUS gives you more information, not less.
> “I’m not trained enough.”
Neither were we the first ten times.
You learn by doing — carefully.
> “Our machine isn’t good enough.”
If you can see black fluid and bright lines, you’re good to go.
---
When T-POCUS is especially clutch:
Acute dyspnoea
Brachycephalic collapse
Suspected pleural effusion
Heart vs lung arguments when referral not an option
Before sedation in a respiratory patient
When radiographs are risky or impossible
[ALL IMAGES ARE THE PROPERTY OF THE CHATTY VETS AND CANNOT BE USED COMMERCIALLY WITHOUT CONSENT]
---


Comments